
EY refers to the global organisation, and may refer to one or more, of the member firms of Ernst & Young Global Limited, each of which is a separate legal entity. Ernst & Young Global Limited, a UK company limited by guarantee, does not provide services to clients.
Recent Searches

The Australian Government has previously succeeded in enacting effective public health legislation. By drawing on international experience, it can introduce further public health laws aimed at achieving targeted improvements in obesity.
In brief:
- The human and economic burden of being overweight or obese is unsustainable. In Australia, the total economic cost of overweight and obesity has been estimated at USD$ 27 billion (AUD$39 billion), or 1.9% of GDP in 2019.1 With the growing prevalence of obesity, especially among children and adolescents, urgent action is needed to change this trend.
- Given the inherent limitations of industry self-regulation, federal legislation is vital to help people make healthier food and drink choices and curb the rise in obesity.
- To improve the likelihood of legislative success, the Government can learn from its own track record in passing population health legislation and consider examples from overseas including Chile on food labelling and advertising, and South Africa on sugar taxation.
1. Obesity is a major public health issue and a leading mortality risk factor
At first glance, Australia appears to be one of the healthiest nations in the world. A newborn can expect to live for 83.1 years, ranking fifth in life expectancy.2 Further, Australia excels in sporting participation and success3 and is widely recognised for its high-quality produce4. Nevertheless, Australia faces an obesity rate of 32%, which is the fifth highest in the world.5
Australia’s obesity crisis has substantial implications for both the healthcare system and economy. In Australia, the direct and indirect economic costs of overweight and obesity were estimated at approximately USD$27 billion (AUD$39 billion), or 1.9% of GDP in 2019.1 These costs are projected to increase to over USD$43 billion (AUD$62 billion) by 2030.1
Physical inactivity and the consumption of food and drink products that are high in sugar, fat and alcohol are major contributors to obesity9 with the high levels of sugar in food and drinks driving chronic disease, in particular diabetes and death.
Being overweight or obese is:
|
Responsible for 8.4% of Australia’s total disease burden.7 |
The leading risk factor contributing to ill health and death (after tobacco).8 |
Linked to a range of other diseases such as type 2 diabetes, hypertensive heart disease, uterine cancer, gout and chronic kidney disease.7 |
|---|
Of most concern is the increasing proportion of children and adolescents aged 5-17 years who are obese and overweight, which has risen from 20% in 1995 to 28% in 2022.7
Being overweight or obese is currently defined by a Body Mass Index (BMI) equal to or more than 25 (overweight) or 30 (obese).9 Whilst recent research indicates BMI-based measures of obesity can sometime underestimate and overestimate a person’s body fat, with further tailoring also required for age, gender and ethnicity,10 this article uses this definition as it is a universally known and understood concept.
Obesity affects lower socioeconomic groups and Aboriginal and Torres Strait Islander peoples more, with obesity rates rising further from cities.9 In 2018–19, approximately two thirds (66.3%) of the non-Aboriginal and Torres Strait Islander adult population were either overweight or obese and more than three-quarters (76.8%) of the Aboriginal and Torres Strait Islander adult population were either overweight (29.6%) or obese (47.2%).11 Worryingly, in 2019, 38% of Aboriginal and Torres Strait Islander children and adolescents were overweight compared to 24% of non-Aboriginal and Torres Strait Islander children.7
There are two key environmental issues underpinning obesity prevalence in Australia:
- Availability and pricing: ‘Fast-foods’ (mass produced and highly processed foods) and sugary drinks are often more available and less expensive than healthier options, particularly in non-metropolitan supermarkets.9 This has contributed to fewer children, especially teenagers, meeting recommended fruit and vegetable intake requirements, with one in six (17%) teenagers consuming at least 5.2kg of sugar each year from sugary drinks alone.12
- Advertising and sponsorship: The high prevalence of fast food, sugary drinks and alcohol promotion in Australian sport and large community events13,14,15 fosters a potential misconception that these products are aligned with a healthy lifestyle. Industry self-regulation through voluntary and variable health labelling standards for food, drinks and alcohol is inadequate and further complicates and compounds this issue. Considering the addictive nature of some of these products16, the parallels with the acceptance of cigarette advertising in popular culture before legal restrictions were enacted are clear.
Australia has committed to the World Health Organization’s (WHO) global target to halt the rise in overweight and obesity, and has developed the National Obesity Strategy 2022-2023 (the Obesity Strategy).9 With obesity rates reaching some of the highest levels ever recorded17, the long term effects and implications are unknown. It is now time to act on obesity to create a healthier and more sustainable Australia.
The recommendations in this article for tackling unhealthy food and sugary drink consumption are also applicable to alcohol. However, given Australia's complex relationship with alcohol18, legislative reforms related to the labelling and promotion of alcoholic beverages are not the primary focus of this article.
2. Obesity requires a systems-wide approach, but legislation is an important lever for change
Over the years, the Australian Government has supported a wide range of health promotion and education programs aimed at reducing obesity, including:
- The National Healthy School Canteens: A national initiative that provides guidelines for healthy foods and drinks supplied in school canteens.
- Shape up Australia: A national initiative that promotes and encourages an evidence-based approach to obesity prevention and aims to reduce confusion about healthy eating and life-style choices.
- Live Lighter: A national initiative that provides tools and resources to support healthy eating habits and an active lifestyle.
Despite this investment, obesity rates have continued to rise due to a myriad of social, economic, political and cultural factors.
Table 1: Examples of external factors influencing obesity
|
Complexity of the stakeholder ecosystem |
Behavioural change challenges |
Complex drivers of obesity |
|---|---|---|
|
Coordination in the design and implementation of policies requires input from many stakeholders across various government sectors and communities. |
Changing long-established eating and physical activity habits requires sustained effort and motivation. |
Obesity is a multifaceted issue influenced by a combination of genetic, environmental, behavioural and social factors. Multipronged strategies are needed that consider these factors holistically. |
|
Complexity of the policy landscape |
Funding and political appetite |
Socioeconomic barriers |
|---|---|---|
|
Coordination across all levels of government and various government sectors is required to support sound decision making, streamlined policy implementation and effective community awareness. |
Investment in preventative health requires many years to materialise, which can deter investment being made where it is needed most. |
Individuals from lower socioeconomic backgrounds may face barriers such as limited access to healthy foods, which health policy design must consider. |
Whilst an increased uptake of weight loss medication (e.g. GLP-1 agonists) may, in time, impact this trend in Australia, they will not ‘treat’ these macro-level drivers. A systems-wide approach is therefore needed to address obesity and involves a comprehensive and coordinated effort that spans multiple sectors and levels of society such as education, culture, physical activity, food and environmental systems.
Although overcoming these factors may take many years, well-designed legislation, as part of this broader approach can be implemented relatively quickly to create a supportive environment for meaningful behavioural change in consumers. This approach aligns with Australia’s Obesity Strategy, which highlights legislative reform and policy change as important universal strategies to positively affect change.
“Universal strategies work to positively shift environments and conditions to create big impacts for everyone, no matter where they live, or their socioeconomic status, cultural identity, gender, age, health or weight status. These include legislative reform and policy change [and] changes to our physical, social and economic environments. These measures can be more effective in reducing inequalities, and do not rely on individual behaviour change.” 9
While the Obesity Strategy does not put any timeframes on introducing such legislative reform, pressure is growing from leading advocacy groups to prioritise legislative solutions that limit food advertising for children and reduce sugar consumption.
2.1 Australia has a good track record in legislating for broader population health issues, such as smoking and e-cigarette use
Population health issues linked to smoking and e-cigarette use, have been successfully addressed through federal legislation, highlighting the opportunity for legislation targeting obesity in Australia.
Table 2: Examples of existing population health related legislation.
Cigarette excise, advertising and packaging legislation | |
Overview | Impact |
The legislation aimed to reduce smoking rates and tobacco related harm through:
|
|
E-cigarette packaging, advertising and importing, manufacturing and supplying legislation | |
The legislation aimed to address the emerging public health challenges associated with e-cigarettes, such as sharply increased use among young people, links to disease and increased likelihood of future cigarette use through:25,26,27
|
|
2.2 Australia can learn from the successes and challenges faced by other countries in addressing obesity through legislative change
Worldwide, various legislative and regulatory measures aimed at combating obesity have been implemented. Successes include Chile’s food labelling and advertising laws, the UK’s co-design approach to advertising restrictions and South Africa’s sugar tax.
Table 3: Case studies of successful international legislation targeting obesity
|
Chile’s Law of Food Labelling and Advertising |
|---|
|
Approximately 40 countries around the world, including Chile, the UK, Ireland, Norway, Mexico, Thailand, and South Korea, already have or are planning to regulate junk food advertising that targets children.28 Of these, Chile’s food advertising and promotion regulation is unique in that it targets the broader Chilean population alongside its focus on children. Importantly, the law extends to advertising that does not relate to a product, such as sport sponsorships and brand advertising.
In 2016, Chile implemented the Law of Food Labelling and Advertising (Ley de Etiqetado), requiring front-of-package warning labels and limiting food advertising to children. This complements existing policies like Chile’s sugar tax on sugary beverages. Packaged foods and drinks with added sugars, saturated fats, or sodium above set limits must display warnings such as “high in [nutrient of concern e.g. sugar]”.29 Additionally, it banned the sale and advertising of such labelled foods in schools and during children’s programming.29,30
A study comparing data from a year before and after the law’s implementation showed a significant decrease in the proportion of unhealthy foods and beverages available for purchase from 51% in 2016 to 44% in 2017.29 Most nutrient and energy reductions were due to manufacturer reformulations to meet the new thresholds and avoid front of packaging (FOP) warning labels.29 The most frequent reformulations were for products high in sugar and sodium.29
Another major outcome was a 23.7% reduction in the purchases of SSBs just one-year post regulation30 with overall calories consumed from purchased beverages decreasing by 7.5%.30 These reductions were larger than those observed from standalone policies, including SSB taxes, previously implemented across Latin America.30 |
|
UK’s Health and Care Act Restricting ‘Less Healthy’ Food and Drink Products |
|---|
|
In 2022, the UK assented to new statutory restrictions on advertising for food and drink products that are high in fat, salt or sugar (HFSS), which will come into force from 1 October 2025. The Act will prohibit HFSS products being advertised between 5:30am and 9pm and it completely prohibits paid-for advertisements of these products online. Although the legislation does not specifically target (sporting) sponsorships, it will reduce the time and means by which HFSS products can sponsor sports and other activities.32 This may encourage these brands to withdraw sponsorships or amend the products advertised.
The aim of these measures is to reduce the: (1) cost of obesity on the National Health Service by lowering obesity related disease rates, particularly in children and (2) health inequalities perpetuated by obesity. It is hoped that the legislation will be successful in meeting these objectives as its design was informed by extensive stakeholder consultation over a four-year period. There is also widespread political support for the law.31 |
|
South Africa’s Health Promotion Levy or ‘Sugar Tax’ |
|---|
|
In 2018, South Africa introduced the Health Promotion Levy (HPL) to combat the rising sugar-intake through SSBs33 and decrease obesity and related health issues, such as diabetes.34 The HPL imposes a tax of approximately 10% on SSBs, with the first four grams of sugar per 100 ml levy free. Any additional sugar content is taxed at 2.1 cents per gram.35
Before the HPL’s implementation, projections indicated a potential 3.8% decline in obesity among South African men and a 2.4% decline among women within a year, potentially reducing the total number of obese adults by over 220,000.36,37
By April 2021, urban households in South Africa had reduced their SSB purchases by 29%, with the sugar content in these beverages decreasing by 51%. Notably, households from lower socioeconomic backgrounds38, reduced their SSB volume and sugar intake by 32% and 57% respectively.39 Approximately 70% of the overall reduction in sugar intake from SSBs was due to behaviour change, with the remaining 30% attributed to reformulation.40
Despite initial concerns, the HPL did not lead to an illicit market of untaxed SSBs. However, a 2021 report revealed that the HPL had resulted in job losses for 16,621 sugar industry employees since its implementation.41 Something to note for Australia given its significant local sugar industry. The HPL was proposed to be extended to pure juice in 2023/2024 and was estimated to incur an additional 5,000 job losses41, this extension is yet to be implemented (as at February 2025). |
Some laws have been less well received, such as Denmark’s fat-tax, from which lessons can also be learned.
Table 4: Case study of unsuccessful international obesity legislation
|
Denmark’s Fat-Tax |
|---|
|
Denmark established the world’s first fat-tax to excise all food items containing saturated fat in 2011. However, it was abolished after only 15 months due to its ‘unbearable burden’ on the country.42
The tax faced heavy criticism and pushback from industry, health professionals and the public due its poor design, lack of input from public health experts, and broad application to staple groceries such as butter and cream.42 The tax led to a 4.7% inflation rise and a 0.8% fall in real wages in its implementation year, costing an estimated 1,300 jobs.42 Many Danes responded by simply purchasing cheaper high-fat products or shopping across the border in Sweden and Germany.43 |
3. Obesity legislation in Australia can tip the balance in changing consumer behaviours
Australia can use obesity legislation to encourage healthier consumer habits and long-term change. Potential legislative levers include labelling regulation, marketing restrictions, taxation, incentives and nutrition standards (Figure 1).
Figure 1: There are a range of legislative levers that can positively influence consumer behaviour
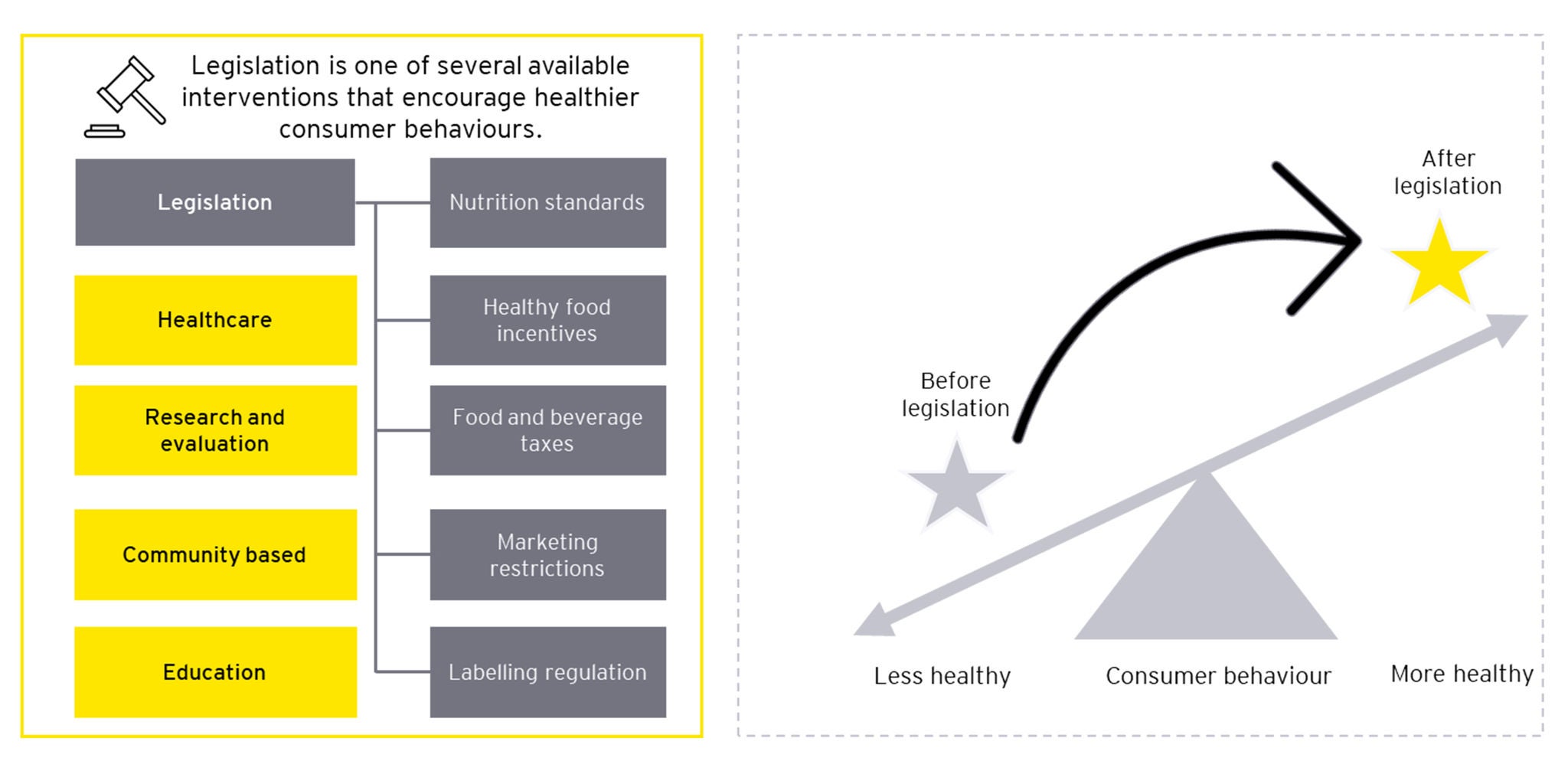
By drawing inspiration from Chile’s Law of Food Labelling and Advertising, Australia should implement FOP warning labels on products with high levels of added sugar, salt, saturated and/or trans fats to improve public awareness of unhealthy food and beverages. The UK’s new advertising laws around HFSS products and Australia’s tobacco plain packaging and advertising laws also provide a precedent for restricting advertising of less healthy products, as well as packaging regulations for unhealthy foods and drinks.
Importantly, advocacy for tougher regulation around unhealthy food and drink advertising, packaging and sponsorship is growing from key stakeholders such as the Food for Health Alliance, which includes the Australian Medical Association (AMA), the Australian Dental Association (ADA), Cancer Council, and many others.44
Emboldened by this support, federal legislation should set ingredient thresholds, as advised by peak bodies and stakeholders, and restrict the advertising and sales of products with FOP warning labels. Banning the sale of products with FOP warning labels to children, prohibiting them in schools, and enforcing advertising restrictions will quickly reduce obesity risk factors, especially for high-risk Australians like children, adolescents, and those from lower socioeconomic backgrounds.
Sugar taxes have been successful in many countries including South Africa, Mexico and the UK45,46 and the use of price to reduce consumption of SSBs, while minimising impacts on disadvantaged populations, is a key objective of the Obesity Strategy. Support for a sugar tax from key stakeholders has been growing for a number of years, with the AMA calling for a tax on a subset of sugary drinks since 2016 via its Sickly-Sweet campaign.47 In 2024, the Cancer Council, Diabetes Australia, the ADA and the AMA welcomed the June 2024 Parliament of Australia’s Diabetes Inquiry recommendations for a levy on sugary drinks.48 However, with a strong local sugar industry, an Australian sugar-tax will need to be nuanced and will be harder to achieve than legislating change on food labelling and advertising.
A sugar tax for SSBs will require close consultation with industry leaders and health experts. Nevertheless, Australia can learn from South Africa’s incremental increase in excise percentage40, which allowed for industry adjustment, reformulation and assessment of legislative impacts at each stage, maintaining strong political will throughout.
3.1 Legislation is not a silver bullet and must be designed carefully to account for broader economic and societal factors
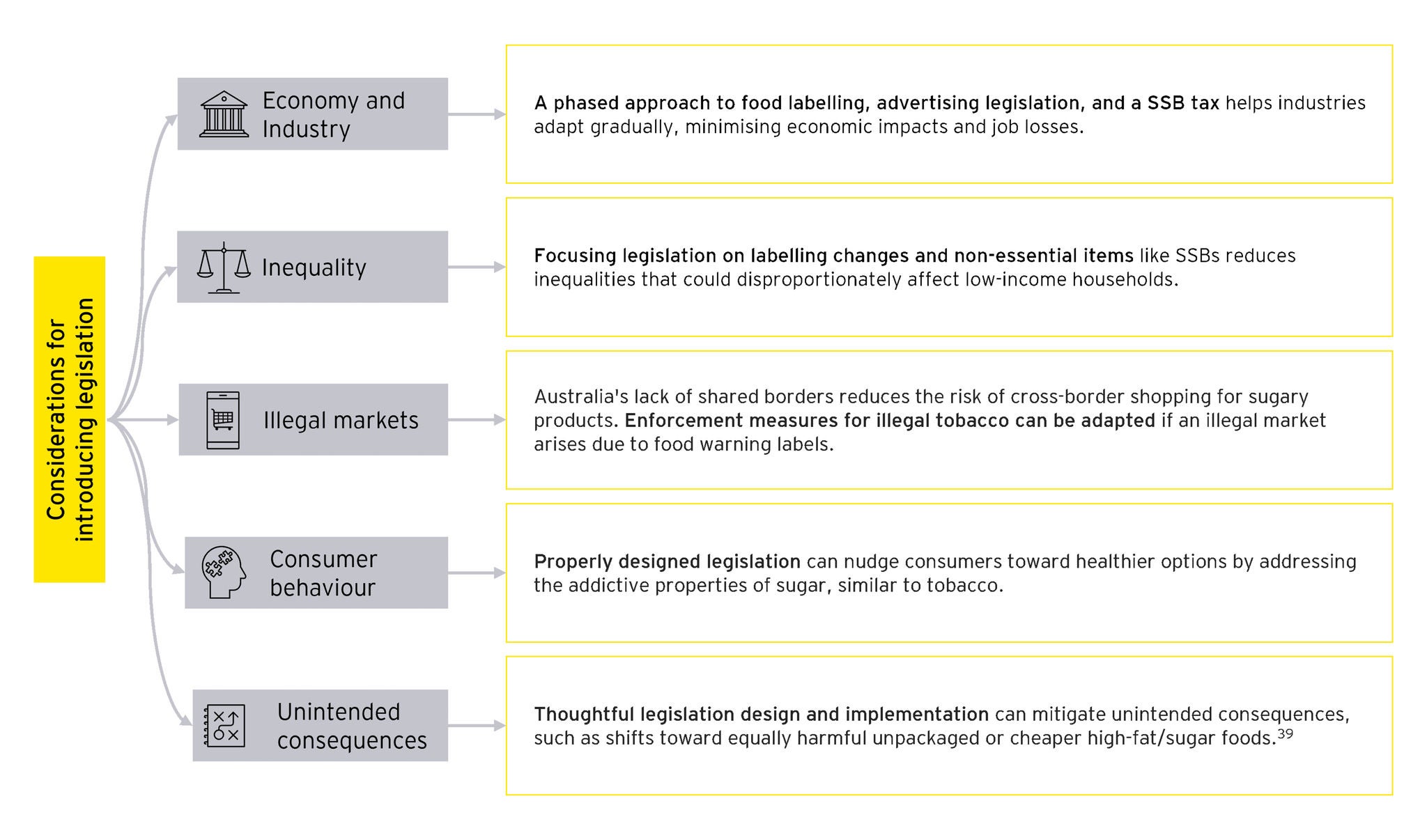
Any significant legislative change can have potential (unforeseen) ripple effects; therefore, several design considerations must be taken into account when implementing food labelling, advertising, and SSB reforms in Australia.
Figure 2: Legislative design considerations
3.2 Legislative change should form part of a systems-wide approach to addressing obesity
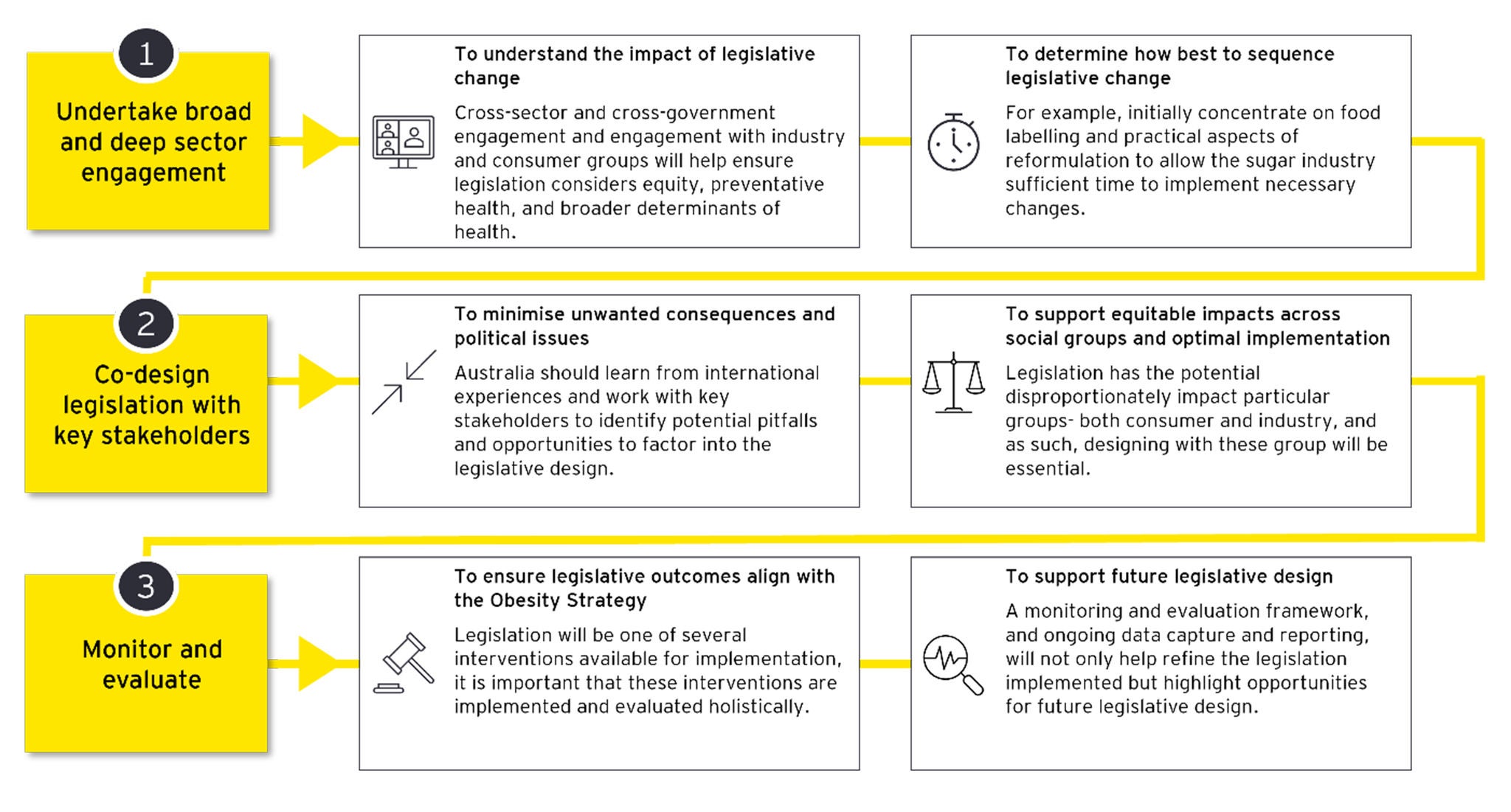
With so many factors influencing the prevalence of obesity, it is essential that legislative changes are implemented as part of a broader systems-wide approach. Such an approach would not only recognise legislation as one of several interventions to pursue but also encourage cross-sector and cross-government collaboration to ensure legislative changes are holistic and sustainable. Given this, political will and stakeholder buy-in will be essential for the success of any new legislation and failing to understand and address community and sector concerns during the design process may lead to strong resistance and ultimate failure.
Figure 3. Implementation considerations that support a systems-wide approach
Summary
By supporting the WHO's objective to halt the rise in diabetes and obesity and developing the Obesity Strategy, the Government has demonstrated its commitment to addressing these public health challenges. Legislation is an important part of the Government's efforts to achieve change. However, it needs to be well designed and considered within the broader systems context and accompanied by strong leadership and engagement with stakeholders. Nevertheless, given the growing pressure on health system sustainability and the broader economic and social impacts of obesity – delaying legislative action incurs a cost that Australia simply cannot afford to ignore.